
FEMORAL TRACTION: EVOLUTION, ENGINEERING, AND SYSTEMS
Femoral traction: Evolution, engineering, and systems
Since Dr. Hugh Owen Thomas (1834-1891) and his “Thomas Splint,” the topic of femoral traction has been a lesson in engineering evolution. It has also been a study of system inertia, because although at least 6 distinct improvements have been made to the original design, the Thomas Splint is still used in numerous medical facilities around the world. And while the concept of traction has been widely adopted, it is still possible to find dangling weights, bricks or sand bottles as shown below. Even in cutting edge institutions, orthopedists will sometimes opt for traction pins drilled through bone to hang weights, rather than employ the newer traction technologies available today.


Sadly, Dr. Thomas did not live to witness the widespread adoption of his splint by the medical community. It took Dr. Thomas’ nephew, Sir Robert Jones, who cared for numerous femur fractures during World War I, to convince the medical establishment that applying traction to a broken femur just might help.
In retrospect, the concept seems so simple. From a structural standpoint, when a femur is fractured, the surrounding musculature lacks internal scaffolding to resist contraction. Like a guitar with a broken neck, or a crane with a broken boom, there is insufficient structure to resist the contracting force. But unlike a broken guitar neck or crane boom, in the case of a femur fracture, muscle contraction further exacerbates the structural failure. Pain and spasms form a feedback loop, and the solution is to provide temporary external scaffolding.
The frequency of femur fractures is extremely variable depending on setting. For example, the military periodically sends thousands of troops jumping from planes, sometimes all at once. Femur fractures are expected and medics plan accordingly. Training is continuous and the quest for the best medical practices and products is never-ending. In other settings, femur fractures are rare events. Practitioners may spend entire careers never applying traction to a single femur. In such settings traction splints may gather dust for years along with MAST trousers, pelvic binders … and that donut shaped magnet that sits in every ER anxiously awaiting any pacemaker gone astray.
For our readers who rarely encounter femur fractures, but who still hope to be prepared, this writing is for you. And for those of you who care for such injuries on a regular basis, we hope that you too will glean some pearls.
Preoperative diagnosis and treatment
We separate preoperative femur fracture management into three distinct phases: Pre-hospital, emergency department, and in-hospital. Unfortunately, specialists in these three areas do not always resonate. But ideally, the approaches chosen by each optimize care for patients in, and between, all three phases.
1. Pre-hospital
Femurs break for a variety of reasons. Some fracture due to compression, for example from sky diving (or rather, after sky diving). Others fracture from torque, perhaps from a caught ski tip. Femurs can snap like tree branches as they wrap around motorcycle handlebars. And they can be blasted apart through penetrating trauma.
For pathologic fractures, the required force may be negligible. Underlying causes for pathologic fracture may include osteoporosis, cancer and infection. Metabolic, medication-related or inborn anomalies may weaken bone as well.
With all types of femur fracture the pain can be immense, and especially so for cases in which the fracture ends are displaced and overlapping. For these, the powerful quadriceps and hamstrings contract virtually unopposed, with intense spasm as the unfortunate result.
First responders often discover patients writhing in pain and simply unable to move. Some patients may be found quite dehydrated having been stranded on the floor for hours. Because the femur is so vascular, it is possible to third-space liters of blood from marrow into the thigh musculature. Hypotensive shock may therefore be present with no sign of external bleeding.
Sometimes patients make the job easy by exclaiming their diagnosis: “I’ve broken my leg… and don’t touch it!” Other times they have underlying comorbidities such as dementia, or concurrent head injuries. Determining the presence of femur injury is hardly challenging. But defining the exact type and location is not simple. Limb shortening and external rotation are strong evidence for femur fracture, while limb shortening and internal rotation suggest hip dislocation. But the location and nature of a fracture or dislocation is rarely certain. In addition, fractures and dislocations may coexist. So treatment for such injuries requires clinical acumen, empathy, finesse… and morphine.
As an aside, regardless of the medical problem, the never-ending debate in the pre-hospital phase is whether to “scoop and run,” vs. treat on scene. Because every scenario is different and transport times may vary widely, the dilemma for responders regarding fractured femurs will probably continue for many years to come. Regardless of protocol, the psychological challenge pre-hospital providers face in treating fractured femurs can be immense. Of course they want to do the best for their patients who may be screaming in agony. But some traction splints lead to far more screaming than others. Combine the screams with the added time to apply traction, the pressure to not donate an expensive piece of equipment to a hospital, and the insecurity that comes with sporadic practice; it makes perfect sense when pre-hospital personnel choose to scoop and run, minus traction.
The act of traction splinting itself can be divided into two parts, traction and splinting. Femoral splinting is easy and can be accomplished with any number of items, the most readily available typically being the uninjured leg. Even for bilateral femur fractures, a great deal of rotational stability may be accomplished simply by wrapping both legs to each other. Useful splinting products for all bones in the body include ACE wraps, Kerlix, towels, sheets, and SAM Splints.
Traction however is the challenge. Many techniques are taught for improvisation in remote, austere settings with sticks, ski poles, paddles and the like. With plenty of time awaiting rescue these techniques are useful.

However the bar is set higher for pre-hospital personnel. Achieving effective traction and stability quickly, with minimal patient movement and pain, is not an easy task. The choice to apply traction or not depends in large part on the pre-hospital provider’s experience, as well as the traction splint available for use.
With or without traction, patients with femur fractures are typically placed on backboards and stretchers. C-collars are often applied as well because fractured femurs are certainly in the realm of “distracting injuries.” Once packaged, patients endure excruciating transports to emergency departments, during which their circulation, sensation and motor function are closely monitored. Pressure points are padded and hopefully pain is controlled with medications and traction readjustments.
On arrival to emergency departments they transition to phase two.
2. Emergency department
Patients with femur fractures are given high priority in emergency departments because they often have concurrent injuries like spine fractures, splenic lacerations, head injuries, etc. They are also at risk for emboli, many are dehydrated, and they may still be experiencing immense pain. On arrival most are left in traction throughout the initial exam. But for a variety of reasons, traction splints are then often removed and replaced with alternative means of stabilization. These are some common reasons to remove traction splints:
- EMS agencies don’t want to lose their expensive equipment. Unlike bicycle share programs in hip cities like Portland and Amsterdam, many medical systems are not yet so refined.
- Emergency physicians need to roll patients to examine their backs, perform rectal exams and to insert Foley catheters. Any splints interfering with these steps must go.
- Bulky traction splints with steel components obscure Xrays and CT images and should be removed.
- Consulting orthopedists often prefer alternative means for splinting.
Orthoglass or plaster are commonly used to replace traction splints in emergency departments. Unfortunately, while these materials make for great splints they offer zero traction. But for the purpose of temporary stabilization through trauma rooms and CT scanners, these options are frequently chosen.
For patients, this transition can be scary and exasperating because they recall the recent pain experienced following injury and with initial splint application. Even for emergency department personnel it may seem absurd to take a patient whose leg is stretched properly, and restart the process.
Ideally patients receive additional analgesia or even femoral nerve blocks prior to this first traction splint transition. Once transitioned, patients are often sent to radiology for further evaluation, and ultimately admitted to either orthopedists or to trauma surgeons for in-hospital treatment.
3. In-hospital
Lucky patients with femur fractures are sent directly from emergency departments to operating rooms for definitive care. Those with less luck are sent to floor beds where they await treatment. In either case, pain control and minimizing complications are top priorities following admission.
Amazingly, those who transition to floor beds may be resplinted yet again! By this time, most have become morphine sponges.
Orthopedists place some in “Bucks traction” or skin traction. The lower limb is wrapped in protective padding and weights applied as shown here:
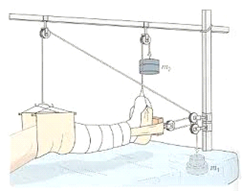

Those who are perhaps least lucky have pins drilled through their distal femurs, tibias or calcanei, from which weights are dangled to maintain traction until more definitive operative care may become available. While this step may seem extreme, it limits the risk of developing pressure points, assures lower limb perfusion, and offers physicians the ability to examine and monitor every square inch of skin.

Specialists in all three phases typically do the best for their patients within the constraints of their respective systems. But from a patient’s perspective, the experience can be exasperating and exhausting.
Of note, the goal of traction is not boney realignment. Some will view Xrays to evaluate the quality of their splinting approach. But during all three phases of preoperative femur fracture care, whether involving buddy wrapped legs, or the Thomas Splint, Bucks traction or traction pins; the primary goals of femoral traction are pain reduction, hemorrhage minimization, and maintained perfusion. Additional objectives are limiting risk for emboli and preventing further damage to underlying tissues.
Traction splint evolution
Having covered the general preoperative femur fracture experience, we will now review the evolution of traction splints. Each splint that exists today has its pros and cons. It is our hope that one day a product will be chosen and systems developed that will enable splint application in the pre-hospital setting, and that will be accepted for use all the way to the operating room, thereby eliminating two painful splint transitions.
1. Thomas splint
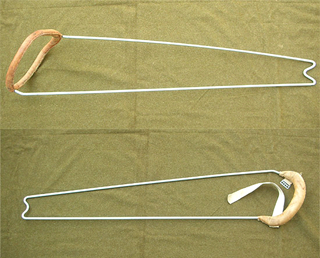
Thomas splints are comprised of a simple steel rod bent to contain, traction and cradle a leg. Straps are used to support and traction the fractured femur. The following photo demonstrates the Thomas “full ring.” A modified version called the “half ring” is also shown, which eliminates the need to slide the ring up the entire injured leg. Dangled weights are not needed for such splints; this represents the first major advancement in traction splinting. Products introduced since the Thomas Splint have embodied incremental improvements, but Drs. Thomas and Jones deserve full credit for their leap in femur fracture management.


2. Hare splint
In the late 1960s Glenn Hare modified the half ring splint by incorporating a ratchet mechanism, and additional means for length adjustment. The ischial pad was also improved. Most importantly, the Hare traction splint provided a more rapid and effective means to actually stretch a femur fracture. Before the Hare, a variety of straps and other creative ankle hitch tensioning techniques were required.
The Hare splint is more compact than the Thomas, as it uses telescoping poles and clamps. Unfortunately the adult version is not compact enough to suit pediatrics, so with the Hare came the first instances of separate pediatric and adult traction splint versions. Today, many EMS services still have protocols that require both pediatric and adult traction splints because of this historical engineering branch point.

Many versions of the Hare splint are still available today.
3. Sager splint
In the early 1970s Joseph Sager and Dr. Anthony Borshneck developed the Sager splint. Rather than steel rods positioned on either side of the fractured limb, the Sager sits between a patient’s legs, and applies traction from the ankle with counter pressure directed onto the ischial tuberosity.
Hare type splints are problematic when used for proximal femur fractures, because the ischial pad may rest directly under the fracture thereby acting as a fulcrum. The Sager splint solves this problem and may be used for any type of femur fracture without concern for fracture location. The Sager also enables traction for bilateral femur fractures.
The Sager also offers ability to measure the actual traction applied. Because of this feature it is now commonly stated that optimal traction is roughly 10-15% of a patient’s body weight (though this estimate may need modification with today’s expanding waistlines). To measure traction force, earlier versions of the splint offered a traction dial, which extended past the foot like the Thomas and Hare. But the most recent Sager is nearly flush with the foot, making it much easier to fit in any type of basket, helicopter or ambulance.
The utility and importance of traction quantification, however, remains debatable. Caregivers today monitor pain, perfusion, skin pressure points and stability far more closely than numerical traction metrics. For those of us who live by “treat the patient, not the numbers,” the traction gauge is superfluous.
The Sager splint is also sold in pediatric and adult versions.

4. Kendrick Traction Device (KTD)
While the Sager was the first monopole splint, the KTD, invented by fire fighter Rick Kendrick in 1986, was the first to move the monopole from medial to lateral leg. For emergency physicians, this greatly improved ease of rolling, rectal examination and Foley insertion. Made from aluminum rather than steel it was the first to claim “relative radiolucency.” It was also the first traction splint to fit every size patient from pediatric to adult.
But the KTD is most notable because it was a major leap in portability. Collapsible like tent poles, and weighing less than 20 ounces, the KTD is easily stored in any pack or vehicle. Bilateral traction is not possible with the KTD, but for those who want to be prepared for such medical calamities, the price of two KTDs remains significantly less than one Sager.

The KTD was a major advancement in traction splinting and remains one of the best-selling traction splints to date.
5. KTD-like splints
Since the KTD patents expired, a variety of similar lateral monopole splints have come to market that are worthy of mention.
a. CT-6
The CT-6 is the most notable KTD-like splint, largely because it is currently in use by the US military. It features a pulley system with 4:1 advantage rather than a simple 1:1 cinch strap. And it is made from carbon fiber. Whether or not carbon fiber is an actual feature remains debatable, because aluminum bends while carbon fiber cracks. But the pulley system is a definite advancement as shown here:

Interestingly, while 4:1 traction is the theoretical mechanical advantage, the experimental traction provided is still less than 1:1. For 40 pounds of force, the output traction is less than 35 pounds. And for the KTD the output is less than 10 pounds. Never underestimate friction!
The CT-6 also offers a single ankle hitch, which fits everything from small limbs to large boots, while the KTD requires a separate boot hitch.
b. ITD (Improved Traction Device)
Built by Emergency Products and Research, the ITD offers a stronger cinch mechanism than the KTD, but with no mechanical advantage. Like the CT-6, the pole sections are made of carbon fiber, and it offers a more padded groin strap. Mid leg straps are labeled.

c. OTD (Optimum Traction Device)
Made by the same company as the ITD, the OTD and the KTD are virtually equivalent.

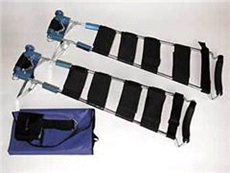
d. TTS (Tactical Traction Splint)North American Rescue has built a black KTD-like splint, which also features labeled midleg straps.

6. STS (Slishman Traction Splint)
In 2007 the current version of the STS was developed by Dr. Sam Slishman, but was only made available in the US by Rescue Essentials in 2012. Like the KTD and its relatives, it is a compact lateral monopole splint. But the major advantages offered by the STS are these:
a. No extension past the foot
This is particularly important for tall patients and for tight transports in baskets, helicopters and ambulances.
b. Proximal traction
All other splints require the rescuer to apply traction distal to the foot. Proximal traction permits rescuers to remain closer to the patient’s head. It also makes traction readjustment easier in tight spaces like helicopters. And it has the side benefit that cooperative and coherent patients are sometimes able to adjust traction to their own fractured femurs to find the position of greatest comfort.
Psychologically this is an enormous advantage because patients can control their own pain. With all other splints, the rescuer-patient interaction goes something like: “As traction is applied to your leg, you may feel discomfort, but eventually you will feel better.” With the STS the dynamic shifts: “Let’s apply traction together until you feel maximum pain relief.” Very different.

c. Useful despite lower leg trauma.
All other traction splints require an intact lower leg to apply traction. For patients with dislocated ankles, tibia fractures, knee sprains, or foot amputations, traction splinting can be impossible. Because the STS ankle hitch may be applied proximal to the calf, or even proximal to the patella, femur traction is still possible.
In addition to the above distinctions, the STS weighs less than 25 ounces, packs compactly, is relatively radiolucent and permits patient rolling, rectal exam, and Foley insertion. Like other lateral monopole splints, it fits all sizes from pediatrics to adults.

Because it is more rigid than KTD-like splints, the STS requires no mid leg straps to maintain traction, though one is provided for rotational stability. For KTD-like splints, the midleg straps keep the splint itself from bowing. The STS is far more rigid with negligible bowing.
Traction in the STS is delivered by an internal pulley mechanism, which offers traction comparable to the CT-6. The input force vs output traction has been tested using more than 80 pounds of input force as shown here:
(The two data sets represent the difference in traction output, depending on which end of the splint is held fixed. Traction applied to a patient, therefore, is somewhere in between, because both distal and proximal ends of the splint move in actual use.)
Other notable traction splints
1. DonwayThe Donway splint is found mainly in British, Australian and New Zealand markets. It most closely resembles the Hare, with 2 telescoping poles and distal traction from the ankle. It also is made with pediatric and adult versions.

Traction is delivered pneumatically rather than mechanically. Groin padding is improved compared to the Hare, and traction can be monitored numerically through a pressure gauge.
For whatever reason, the Donway splint never found its way into US markets. Given recent advances in splinting, the prognosis for the Donway seems poor.
2. Level One Trauma Splint “LOTS”
The LOTS is unusual because it employs a carbon fiber rod positioned posterior to the injured leg. It also utilizes a material wrap with Velcro straps to completely splint the leg. Traction is from the foot and, like the KTD, the LOTS utilizes a 1:1 cinch strap. It is meant to be useful for splinting other types of fractures, and is sold with a pelvic binder as well.

For the purpose of splinting any limb injury, the LOTS is an exceptional product. But for traction, it suffers because of the added time for application, and because it limits access to the injured limb. Expense is also a limiting factor.
3. REEL
Perhaps the strongest, most “bomb-proof” splint to date, the Reel is also the most expensive. Another variant of the Hare, the Reel features numerous points of articulation enabling position of injury splinting for arms and legs. Fear of exacerbating injuries made the existence of the Reel splint possible years ago. But today pre-hospital providers are more empowered and encouraged to align injuries on scene for transport, thereby greatly diminishing a need for the Reel.


Similar to the Hare, the Reel features two articulating parallel poles, a ratchet mechanism, numerous midleg straps and handles to facilitate lifting. It is however, quite bulky and radio-opaque. The Reel may have a role in military settings for long transports. But in all other scenarios it offers no appreciable advantage.
3. Slishman ski pole
The current STS has been evolving since the late 1990s and originates from a collapsible ski pole. The original ski pole version utilized the same pulley mechanism found in today’s STS and also boasted shoulder “self-reduction” capability. While useful for ski patrollers and expedition leaders, the multi-use traction splint is less desirable in EMS and hospital markets, largely because of the added expense and the likelihood for loss or theft.


Conclusion
Perhaps one day we will pour a rapidly curing Kevlar polymer over all fractures creating a bullet-proof exoskeleton. Maybe femoral nails and external fixators will be displaced by rapid bone regeneration substances injected intraosseously. But until that time, traction splints will continue to evolve and we will continue to utilize external thigh-stretching techniques and products.
As traction splints become simpler and easier to apply, maybe the dilemma of scoop and run vs. treat on scene will fade a bit for femur fractures. Back when Hare or Thomas splints were the only options, the decision to give morphine, wrap quick and drive fast probably made the most sense. Added pain and time lost with application of these splints was not worth the trouble, especially in settings where local emergency departments would likely remove them.
Today with simpler and less expensive KTD-like splints and the STS, on-scene traction will hopefully be the path chosen more frequently.
Dr. Slishman hopes that one day his splint will be applied in the field and left in place all the way to the operating room, thereby eliminating the two painful preoperative splint transitions as well. In fact, he claims to have used his splint on many of his own patients with no reported complications. Following the 2010 Haiti earthquake, the STS was applied to more than 7 patients for up to 10 days (only 7 because that’s all he brought.) Apparently his patients were quite willing and able to modify traction on their own limbs. But Dr. Slishman stresses that he is naturally biased and that his patients received “above average” attention. Further study on prolonged application is clearly required.
As for application of the STS ankle hitch proximal to the calf, since this is truly possible, it could one day become standard. But given the time it took for the Thomas splint to gain favor, and the fact that it still remains in use today despite numerous significant splint improvements, Dr. Slishman feels that the proximal calf approach could take another century.
In the meantime, if you break your femur, first demand morphine. Second, offer to buy the splint. And third, don’t let anyone remove it until the OR!